Recurrent Wheezing in an Infant
Radiology Cases in Pediatric Emergency Medicine
Volume 6, Case 17
Meta Lee, MD
Queen's Medical Center
Kapiolani Medical Center For Women And Children
University of Hawaii John A. Burns School of Medicine
A 10 month old male comes to the ED with a chief
complaint of wheezing and coughing for one day. He
has just flown in from the Marshall Islands with his
parents and an interpreter, who are not available at this
time. He has no fever, vomiting or diarrhea. Despite
the language barrier you are able to elicit that the
patient has had similar coughing and wheezing
episodes in the past.
Exam: VS T37.1 (tympanic), P120, R58, oxygen
saturation 100% (room air). He is noted to be in mild
respiratory distress with audible wheezes,
mild-moderate retractions, moist expiratory rhonchi and
crackles diffusely.
He is given an albuterol nebulizer treatment with
marked improvement in symptoms. His respiratory rate
decreases, his retractions resolve, his aeration
improves and his breath sounds clear except for a slight
decrease in aeration on the left.
His mother communicates that he is to see a doctor
the following day, and you decide to discharge the
patient on albuterol syrup with instructions to follow-up
with this physician in the morning.
The next day he comes to the clinic with his
interpreter, who has a copy of his medical records from
the Marshall Islands. He has had a history of recurrent
episodes of wheezing and cough with respiratory
distress for which he has been hospitalized at 1, 3 and
4 months of age. His mother indicates that he is doing
much better since his ED visit last night. A chest
radiograph is ordered.
View his chest radiographs.
PA view.
 Lateral view.
Lateral view.
 The PA view demonstrates decreased pulmonary
vascularity and hyperlucency of the left lung. His right
lung demonstrates increased pulmonary vascularity.
The lateral view demonstrates a mass effect posterior
to the lower portion of the trachea, which compresses
and bows the trachea anteriorly with considerable
narrowing of the inferior portion of the trachea and left
main bronchus. These findings are suspicious for a
large mediastinal mass which is compressing the lower
trachea and mainstem bronchus causing obstructive
emphysema of the left lung and decreased perfusion of
this lung. A barium esophagram is ordered.
View esophagram.
AP view.
The PA view demonstrates decreased pulmonary
vascularity and hyperlucency of the left lung. His right
lung demonstrates increased pulmonary vascularity.
The lateral view demonstrates a mass effect posterior
to the lower portion of the trachea, which compresses
and bows the trachea anteriorly with considerable
narrowing of the inferior portion of the trachea and left
main bronchus. These findings are suspicious for a
large mediastinal mass which is compressing the lower
trachea and mainstem bronchus causing obstructive
emphysema of the left lung and decreased perfusion of
this lung. A barium esophagram is ordered.
View esophagram.
AP view.
 Lateral view.
Lateral view.
 Barium is hand injected into the proximal esophagus
through a nasogastric tube. The esophagus is
displaced laterally as seen on the AP view. The lateral
view demonstrates the mass located between the
trachea (the tracheal air column is compressed and
displaced anteriorly) and the barium filled esophagus
(which is displaced posteriorly). A CT scan of the chest
is ordered.
View CT scan.
Barium is hand injected into the proximal esophagus
through a nasogastric tube. The esophagus is
displaced laterally as seen on the AP view. The lateral
view demonstrates the mass located between the
trachea (the tracheal air column is compressed and
displaced anteriorly) and the barium filled esophagus
(which is displaced posteriorly). A CT scan of the chest
is ordered.
View CT scan.
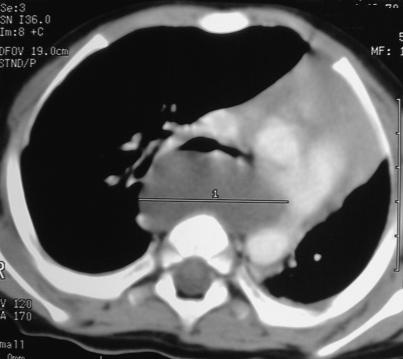 There is a 4.5 x 4.5 x 2.5 cm cystic mass posterior
to the trachea and the mainstem bronchi. The mass
causes marked narrowing of the left main bronchus.
The esophagus is displaced to the patient's right by the
mass with flattening of the esophageal lumen. This
mass is most likely a mediastinal bronchogenic cyst.
An esophageal duplication cyst could have a similar
appearance.
The patient underwent surgical excision of the
mediastinal mass via thoracotomy without
complications. Pathology confirmed the mass to be a
bronchogenic cyst.
Discussion
Bronchogenic cysts represent 10-20% of congenital
cystic diseases of the lung, and account for
approximately 10% of mediastinal masses. These
cysts are the result of ectopic budding of the
tracheobronchial tree during embryologic development
from the primitive foregut. Histologically, these cysts
are composed of tissue normally found in the trachea
and bronchi (mucous glands, smooth muscle, elastic
tissue and usually cartilage). Fluid found within is
mucoid and clear or white, unless hemorrhage has
occurred, in which case the contents are thick and
brown. Calcium crystals may also be seen. Because
these cysts form before the development of alveoli,
there is no gas exchange potential, even if
communication exists.
Bronchogenic cysts can be classified by location:
paratracheal, carinal, paraesophageal, hilar and
miscellaneous. The majority of bronchogenic cysts are
either attached to the tracheobronchial tree by a stalk of
fibrous tissue or are embedded in the wall of the
trachea or bronchus. Less frequently, there may be
communication with the respiratory tract, resulting in
progressive dilatation with air, resulting in atelectasis,
recurrent infection and mediastinal shift.
Clinically, the majority of bronchogenic cysts are
symptomatic and occur in infancy or early childhood.
Respiratory distress is the most common presentation
in pediatric patients, manifested by recurring episodes
of cough, stridor, wheezing and retractions. In later
childhood or adulthood, bronchogenic cysts are more
commonly asymptomatic, with symptoms eventually
developing due to increasing size of the cyst. Chest
pain, cough and dyspnea are the most common
complaints in adults. Persistent or recurrent
pneumonia, abscess or empyema can occur at any age
as a result of impaired clearance of secretions past the
cyst, or infection, or rupture of the cyst itself.
Diagnostically, bronchogenic cysts can be identified
on plain chest radiographs in up to two thirds of cases
in any age group. The radiographic appearance
depends on whether the cyst is air filled, fluid filled, or
air and fluid filled. An air filled cyst has the appearance
of a pneumatocele. Completely fluid filled cysts cannot
be discriminated from solid masses on plain film. The
presence of air-fluid levels on erect or decubitus films
imply tracheobronchial communication and active
infection, which can be difficult to distinguish from a
lung abscess. Bronchogenic cysts may not be visible
on chest radiographs due to surrounding mediastinal
structures and inflammation. Hyperinflation,
pneumonitis, atelectasis, mediastinal deviation, or
abnormal separation of the trachea and esophagus may
impede the radiographic visibility of a bronchogenic
cyst. Computed tomography helps to better define the
cyst in terms of fluid content, wall thickness, solitary or
multiple nature, location and other findings.
Treatment options for bronchogenic cysts include
observation, resection and aspiration. All symptomatic
or enlarging cysts should be resected. Infected cysts
should be removed once tissue levels of
broad-spectrum antibiotics have been established. In
poor surgical candidates, aspiration of a cyst can be
done to confirm a benign diagnosis. Instillation of a
sclerosing agent is another therapeutic option.
Asymptomatic simple cysts, if observed, have the
potential to grow and can result in higher rates of
perioperative complications once becoming
symptomatic. There is also a rare association of
bronchogenic cysts with rhabdomyosarcoma.
References
1. Coran A, Drongowski R. Congenital Cystic
Disease of the Tracheobronchial Tree in Infants and
Children - Experience with 44 Consecutive Cases.
Archives of Surgery 1994;129:521-527.
2. Decamp M. Congenital Cysts of the
Mediastinum: Bronchopulmonary Foregut Anomalies.
In: Fishman A (ed). Pulmonary Diseases and
Disorders, third edition. New York, NY, McGraw-Hill
Companies, Inc., 1998, pp. 1499-1506.
3. Freundlich I, Bragg D. Cysts and Cavities of the
Lung. In: Freundlich I, Bragg D (eds). A Radiographic
Approach to Diseases of the Chest. Baltimore, MD,
Williams and Wilkins, 1992, pp. 93-99.
4. Haddon M, Bowen A. Bronchopulmonary and
Neurenteric Forms of Foregut Anomalies - Imaging for
Diagnosis and Management. Radiology Clinics of North
America 1991;29(2):241-251.
5. Lierl M. Congenital Abnormalities. In: Hilman B
(ed). Pediatric Respiratory Disease: Diagnosis and
Treatment. Philadelphia, PA, W.B. Saunders
Company, 1993, pp. 457-461.
There is a 4.5 x 4.5 x 2.5 cm cystic mass posterior
to the trachea and the mainstem bronchi. The mass
causes marked narrowing of the left main bronchus.
The esophagus is displaced to the patient's right by the
mass with flattening of the esophageal lumen. This
mass is most likely a mediastinal bronchogenic cyst.
An esophageal duplication cyst could have a similar
appearance.
The patient underwent surgical excision of the
mediastinal mass via thoracotomy without
complications. Pathology confirmed the mass to be a
bronchogenic cyst.
Discussion
Bronchogenic cysts represent 10-20% of congenital
cystic diseases of the lung, and account for
approximately 10% of mediastinal masses. These
cysts are the result of ectopic budding of the
tracheobronchial tree during embryologic development
from the primitive foregut. Histologically, these cysts
are composed of tissue normally found in the trachea
and bronchi (mucous glands, smooth muscle, elastic
tissue and usually cartilage). Fluid found within is
mucoid and clear or white, unless hemorrhage has
occurred, in which case the contents are thick and
brown. Calcium crystals may also be seen. Because
these cysts form before the development of alveoli,
there is no gas exchange potential, even if
communication exists.
Bronchogenic cysts can be classified by location:
paratracheal, carinal, paraesophageal, hilar and
miscellaneous. The majority of bronchogenic cysts are
either attached to the tracheobronchial tree by a stalk of
fibrous tissue or are embedded in the wall of the
trachea or bronchus. Less frequently, there may be
communication with the respiratory tract, resulting in
progressive dilatation with air, resulting in atelectasis,
recurrent infection and mediastinal shift.
Clinically, the majority of bronchogenic cysts are
symptomatic and occur in infancy or early childhood.
Respiratory distress is the most common presentation
in pediatric patients, manifested by recurring episodes
of cough, stridor, wheezing and retractions. In later
childhood or adulthood, bronchogenic cysts are more
commonly asymptomatic, with symptoms eventually
developing due to increasing size of the cyst. Chest
pain, cough and dyspnea are the most common
complaints in adults. Persistent or recurrent
pneumonia, abscess or empyema can occur at any age
as a result of impaired clearance of secretions past the
cyst, or infection, or rupture of the cyst itself.
Diagnostically, bronchogenic cysts can be identified
on plain chest radiographs in up to two thirds of cases
in any age group. The radiographic appearance
depends on whether the cyst is air filled, fluid filled, or
air and fluid filled. An air filled cyst has the appearance
of a pneumatocele. Completely fluid filled cysts cannot
be discriminated from solid masses on plain film. The
presence of air-fluid levels on erect or decubitus films
imply tracheobronchial communication and active
infection, which can be difficult to distinguish from a
lung abscess. Bronchogenic cysts may not be visible
on chest radiographs due to surrounding mediastinal
structures and inflammation. Hyperinflation,
pneumonitis, atelectasis, mediastinal deviation, or
abnormal separation of the trachea and esophagus may
impede the radiographic visibility of a bronchogenic
cyst. Computed tomography helps to better define the
cyst in terms of fluid content, wall thickness, solitary or
multiple nature, location and other findings.
Treatment options for bronchogenic cysts include
observation, resection and aspiration. All symptomatic
or enlarging cysts should be resected. Infected cysts
should be removed once tissue levels of
broad-spectrum antibiotics have been established. In
poor surgical candidates, aspiration of a cyst can be
done to confirm a benign diagnosis. Instillation of a
sclerosing agent is another therapeutic option.
Asymptomatic simple cysts, if observed, have the
potential to grow and can result in higher rates of
perioperative complications once becoming
symptomatic. There is also a rare association of
bronchogenic cysts with rhabdomyosarcoma.
References
1. Coran A, Drongowski R. Congenital Cystic
Disease of the Tracheobronchial Tree in Infants and
Children - Experience with 44 Consecutive Cases.
Archives of Surgery 1994;129:521-527.
2. Decamp M. Congenital Cysts of the
Mediastinum: Bronchopulmonary Foregut Anomalies.
In: Fishman A (ed). Pulmonary Diseases and
Disorders, third edition. New York, NY, McGraw-Hill
Companies, Inc., 1998, pp. 1499-1506.
3. Freundlich I, Bragg D. Cysts and Cavities of the
Lung. In: Freundlich I, Bragg D (eds). A Radiographic
Approach to Diseases of the Chest. Baltimore, MD,
Williams and Wilkins, 1992, pp. 93-99.
4. Haddon M, Bowen A. Bronchopulmonary and
Neurenteric Forms of Foregut Anomalies - Imaging for
Diagnosis and Management. Radiology Clinics of North
America 1991;29(2):241-251.
5. Lierl M. Congenital Abnormalities. In: Hilman B
(ed). Pediatric Respiratory Disease: Diagnosis and
Treatment. Philadelphia, PA, W.B. Saunders
Company, 1993, pp. 457-461.
Return to Radiology Cases In Ped Emerg Med Case Selection Page
Return to Univ. Hawaii Dept. Pediatrics Home Page