Infant Skull Fractures
Radiology Cases in Pediatric Emergency Medicine
Volume 5, Case 9
Loren G. Yamamoto, MD, MPH
Kapiolani Medical Center For Women And Children
University of Hawaii John A. Burns School of Medicine
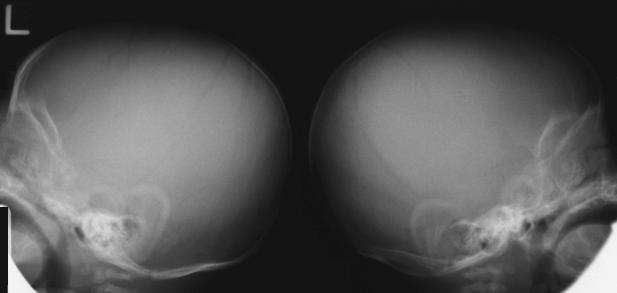
Plain film radiographs of the skull are obtained in
limited circumstances. In most instances, CT scanning
of the head is more useful. Some hospitals and clinics
do not have easy access to CT scanning and hence,
they rely more on the use of clinical assessment, plain
film skull radiographs, and judicious referral to a center
with a CT scanner. Interpreting skull radiographs in
infants can be difficult since their skulls have many
normal lucencies. Sutures are generally sinusoidal in
appearance and in their standard anatomic locations
(coronal, sagittal, and labdoidal). Fractures are rarely
sinusoidal. Fractures are usually linear, stellate, or
depressed.
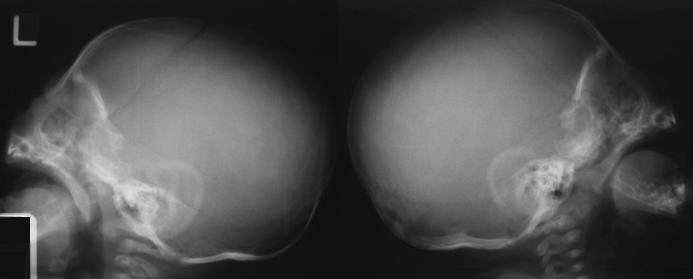
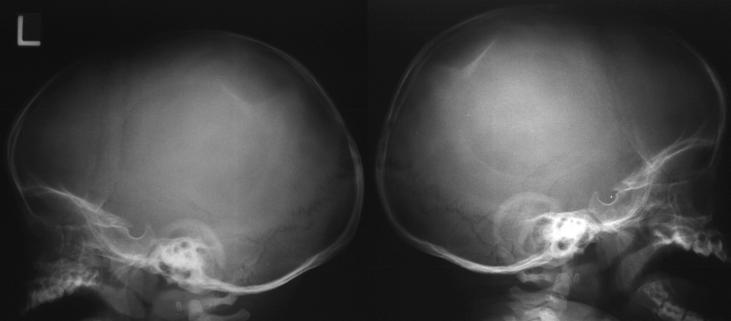
View normal skull radiograph.

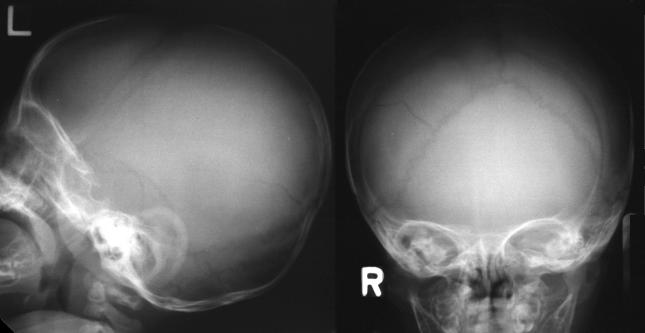
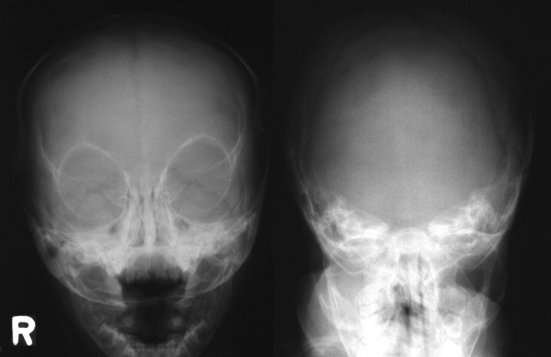
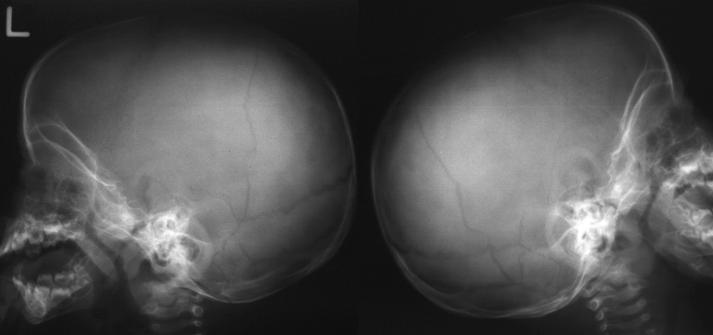
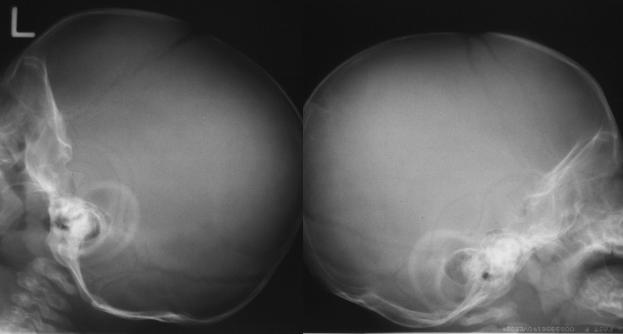 Four standard views are often obtained. An AP
view, a Towne's view, and two lateral views. The
Towne's view is an AP view with the neck flexed
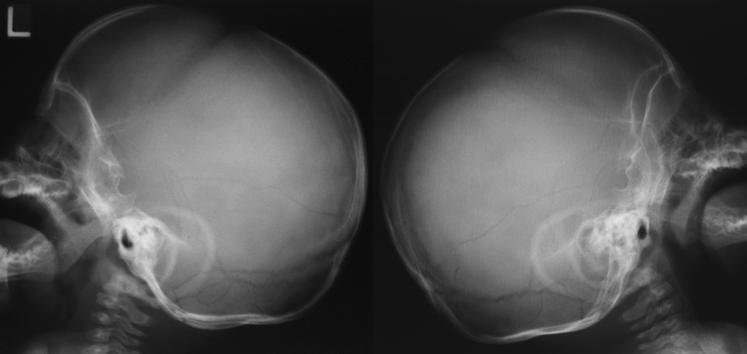
forward. Two lateral views can be more optimal than a
single lateral view to permit the film to focus on one
side at a time.
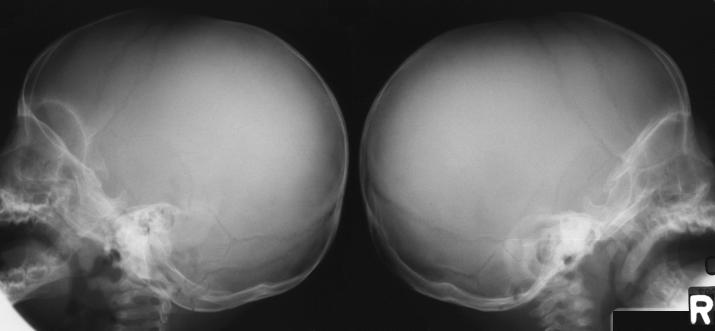
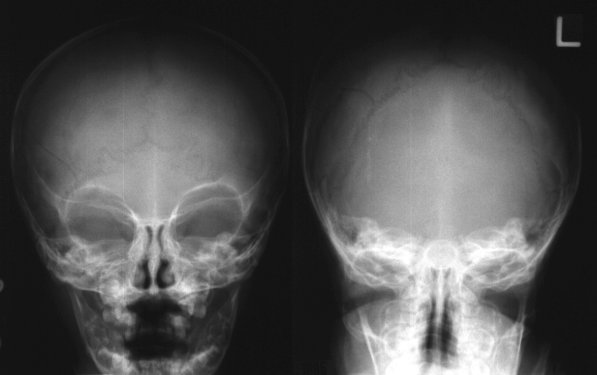
Locate the coronal, sagittal, and lambdoidal sutures
on these skull radiographs. In addition to these major
sutures, the anterior fontanelle is often visible. A suture
extends from the anterior tip of the anterior fontanelle
into the frontal bone. Two smaller sutures on each side
of the skull are present in the lower skull adjacent to the
mastoid; the parietomastoid suture and the
occipitomastoid suture.
View the locations of these sutures.
Four standard views are often obtained. An AP
view, a Towne's view, and two lateral views. The
Towne's view is an AP view with the neck flexed
forward. Two lateral views can be more optimal than a
single lateral view to permit the film to focus on one
side at a time.
Locate the coronal, sagittal, and lambdoidal sutures
on these skull radiographs. In addition to these major
sutures, the anterior fontanelle is often visible. A suture
extends from the anterior tip of the anterior fontanelle
into the frontal bone. Two smaller sutures on each side
of the skull are present in the lower skull adjacent to the
mastoid; the parietomastoid suture and the
occipitomastoid suture.
View the locations of these sutures.
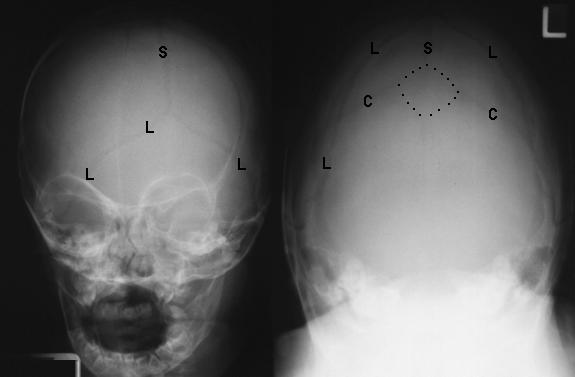
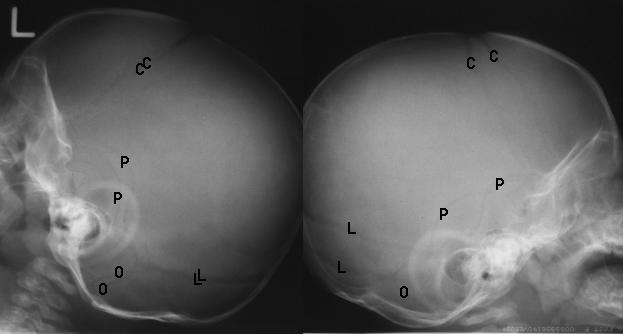 C - Coronal
S - Sagittal
L - Lambdoidal
P - Parietomastoid (squamosal)
O - Occipitomastoid
The anterior fontanelle is outlined in the broken line.
Note that a suture extends anteriorly into the frontal
bone from the anterior tip of the anterior fontanelle.
Linear skull fractures are rarely associated with the
need for neurosurgical intervention. They will often
present to an acute care clinic or emergency
department several days after the injury with a
subgaleal hematoma (soft swelling on the side of the
head) as a chief complaint. These are benign and
should not be aspirated unless an infection is present.
Parietal skull fractures which cross the path of the
middle meningeal artery or other major vessels may be
associated with epidural or other types of intracranial
hemorrhage. In young children, the middle meningeal
artery does not groove into the bone as it does in adults
and thus, laceration of the middle meningeal artery is
less likely to occur (compared to adults) with a parietal
skull fracture. Roughly half of the epidural hematomas
in children occur in the absence of skull fractures.
Thus, plain film skull radiographs should not be used as
a routine screening measure to determine risk of
intracranial hemorrhage. CT scanning is more effective
at ruling out cerebral hemorrhages.
Neither CT nor plain film skull radiographs are highly
reliable in ruling out a basilar skull fracture. Such
fractures are difficult to see on CT scans and plain film
skull radiographs. This diagnosis is often made
clinically (nasal CSF leak, CSF otorrhea,
hemotympanum, Battle's sign, etc.) and then confirmed
on fine or angled CT cuts, or MRI.
Widely separated linear skull fractures (widely
diastatic) are associated with a higher risk of subdural
hematoma and an increased risk of developing
leptomeningeal cysts. The follow-up radiograph one
month later may show a "growing" fracture that results
from a meningeal laceration. This results in a bulging
leptomeningeal sac that causes erosion of the overlying
skull and an eventual skull defect if it is not repaired.
Depressed skull fractures may be evident on plain
radiographs, however, CT scanning is better able to
determine the extent of depression.
View the plain film skull radiographs to test your skill
in interpreting these radiographs.
View Case B.
C - Coronal
S - Sagittal
L - Lambdoidal
P - Parietomastoid (squamosal)
O - Occipitomastoid
The anterior fontanelle is outlined in the broken line.
Note that a suture extends anteriorly into the frontal
bone from the anterior tip of the anterior fontanelle.
Linear skull fractures are rarely associated with the
need for neurosurgical intervention. They will often
present to an acute care clinic or emergency
department several days after the injury with a
subgaleal hematoma (soft swelling on the side of the
head) as a chief complaint. These are benign and
should not be aspirated unless an infection is present.
Parietal skull fractures which cross the path of the
middle meningeal artery or other major vessels may be
associated with epidural or other types of intracranial
hemorrhage. In young children, the middle meningeal
artery does not groove into the bone as it does in adults
and thus, laceration of the middle meningeal artery is
less likely to occur (compared to adults) with a parietal
skull fracture. Roughly half of the epidural hematomas
in children occur in the absence of skull fractures.
Thus, plain film skull radiographs should not be used as
a routine screening measure to determine risk of
intracranial hemorrhage. CT scanning is more effective
at ruling out cerebral hemorrhages.
Neither CT nor plain film skull radiographs are highly
reliable in ruling out a basilar skull fracture. Such
fractures are difficult to see on CT scans and plain film
skull radiographs. This diagnosis is often made
clinically (nasal CSF leak, CSF otorrhea,
hemotympanum, Battle's sign, etc.) and then confirmed
on fine or angled CT cuts, or MRI.
Widely separated linear skull fractures (widely
diastatic) are associated with a higher risk of subdural
hematoma and an increased risk of developing
leptomeningeal cysts. The follow-up radiograph one
month later may show a "growing" fracture that results
from a meningeal laceration. This results in a bulging
leptomeningeal sac that causes erosion of the overlying
skull and an eventual skull defect if it is not repaired.
Depressed skull fractures may be evident on plain
radiographs, however, CT scanning is better able to
determine the extent of depression.
View the plain film skull radiographs to test your skill
in interpreting these radiographs.
View Case B.

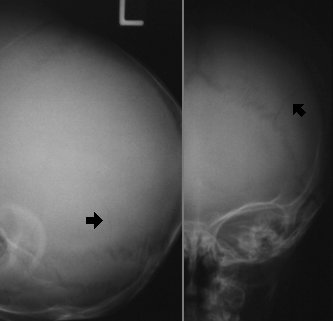
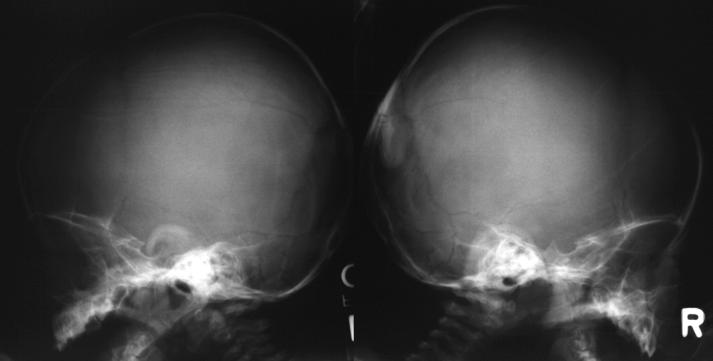 This 11-month old infant fell and struck his head on
a hard surface.
Case B Interpretation:
Linear fracture of the posterior portion of the right
parietal bone extending across the lambdoidal suture
into the occipital bone.
This 11-month old infant fell and struck his head on
a hard surface.
Case B Interpretation:
Linear fracture of the posterior portion of the right
parietal bone extending across the lambdoidal suture
into the occipital bone.
 View Case C.
View Case C.
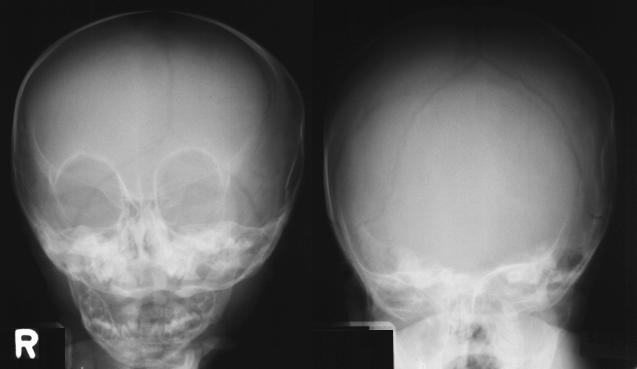
 The history in this case is that this 2-month old fell
off a bed twice. It should be noted that this history is
highly suspicious. A 2-month old infant cannot move
about very much. While it may be possible for this
2-month old infant to have fallen off a bed once, it is
very unlikely that any parent would have allowed this to
occur twice on the same day.
Case C Interpretation:
Right parietal skull fracture.
The history in this case is that this 2-month old fell
off a bed twice. It should be noted that this history is
highly suspicious. A 2-month old infant cannot move
about very much. While it may be possible for this
2-month old infant to have fallen off a bed once, it is
very unlikely that any parent would have allowed this to
occur twice on the same day.
Case C Interpretation:
Right parietal skull fracture.
 View Case D.
View Case D.

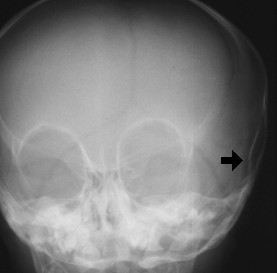
 The mother of this 2-month infant fell onto a hard
surface while she was carrying her infant.
Case D Interpretation:
Linear fracture of the right occiput.
The mother of this 2-month infant fell onto a hard
surface while she was carrying her infant.
Case D Interpretation:
Linear fracture of the right occiput.
 View Case E.
View Case E.

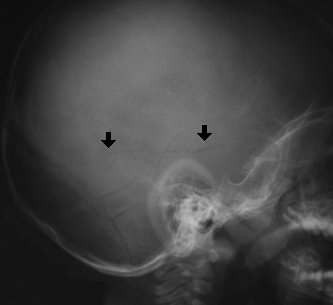
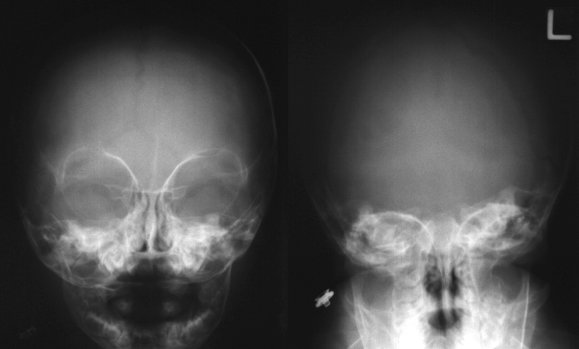
 This 13-month old infant was noted to have a soft
swelling on his head two days following an episode of
head trauma following which, his behavior was normal.
Case E Interpretation:
Horizontal hairline fracture (very subtle) running
across the left temporal bone which extends posteriorly
to the level of the labdoidal suture.
This 13-month old infant was noted to have a soft
swelling on his head two days following an episode of
head trauma following which, his behavior was normal.
Case E Interpretation:
Horizontal hairline fracture (very subtle) running
across the left temporal bone which extends posteriorly
to the level of the labdoidal suture.
 View Case F.
View Case F.
 Case F Interpretation:
There is a depressed skull fracture over the
posterior right parietal bone. The hyperdense
(sclerotic) appearance of the skull abnormality indicates
the presence of a depressed skull fracture.
Case F Interpretation:
There is a depressed skull fracture over the
posterior right parietal bone. The hyperdense
(sclerotic) appearance of the skull abnormality indicates
the presence of a depressed skull fracture.
 View Case G.
View Case G.
 Case G Interpretation:
There is a 3 cm angled fracture in the right parietal
bone which communicates with the labdoidal suture.
Case G Interpretation:
There is a 3 cm angled fracture in the right parietal
bone which communicates with the labdoidal suture.
 View Case H.
View Case H.

 Case H Interpretation:
Linear skull fracture of the right parietal bone
extending from the labdoidal suture to the
parietomastoid suture.
Case H Interpretation:
Linear skull fracture of the right parietal bone
extending from the labdoidal suture to the
parietomastoid suture.
 View Case I.
View Case I.
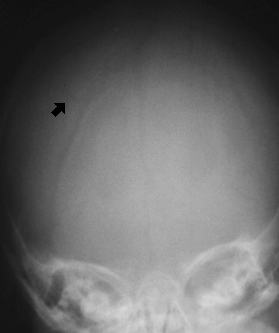
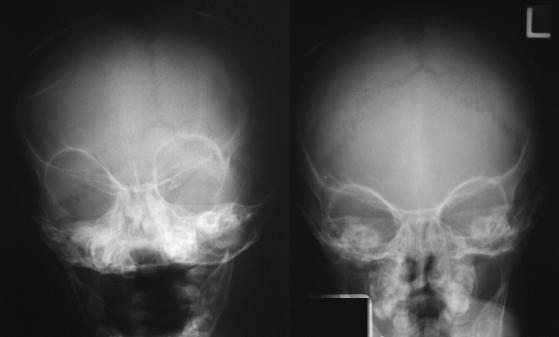
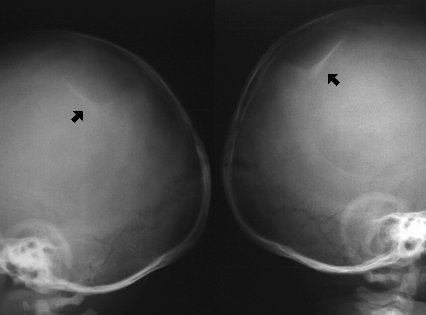
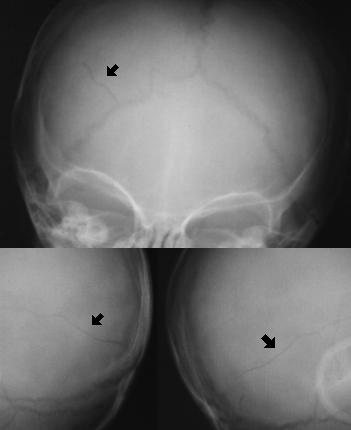
 Case I Interpretation:
There is a short parietal skull fracture (very subtle)
near the vertex of the skull. It is difficult to lateralize on
the frontal views. It is probably on the left.
Case I Interpretation:
There is a short parietal skull fracture (very subtle)
near the vertex of the skull. It is difficult to lateralize on
the frontal views. It is probably on the left.
 View Case J.
View Case J.
 Case J Interpretation:
There is a fracture of the lower portion of the left
parietal bone.
Case J Interpretation:
There is a fracture of the lower portion of the left
parietal bone.
 View Case K.
View Case K.
 Case K Interpretation:
Long linear left parietal fracture extending from the
vertex to the labdoidal suture.
Case K Interpretation:
Long linear left parietal fracture extending from the
vertex to the labdoidal suture.
 View Case L.
View Case L.
 Case L Interpretation:
Linear fracture extending the length of the right
parietal bone.
Case L Interpretation:
Linear fracture extending the length of the right
parietal bone.
 View Case M.
View Case M.

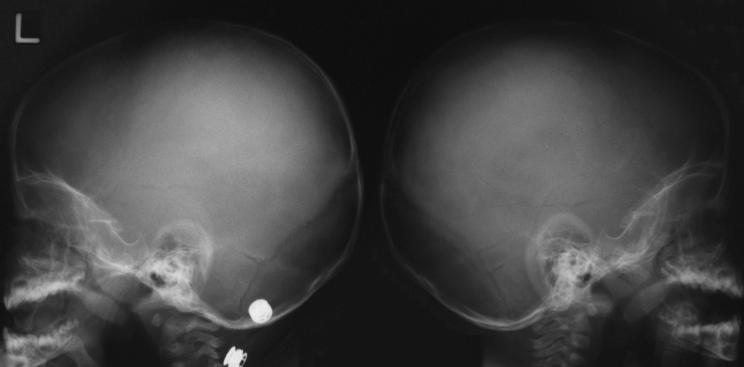
 Case M Interpretation:
Biparietal skull fractures.
Case M Interpretation:
Biparietal skull fractures.
 View Case N.
View Case N.

 Case N Interpretation:
Linear fracture of the posterior left parietal region.
Case N Interpretation:
Linear fracture of the posterior left parietal region.
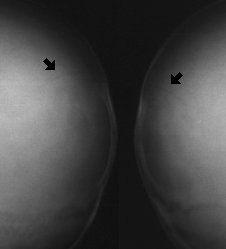
 View Case O.
View Case O.
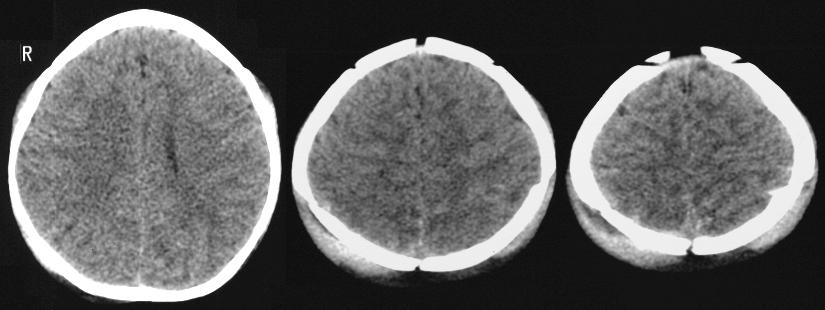
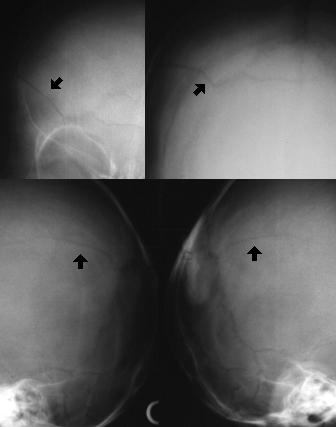
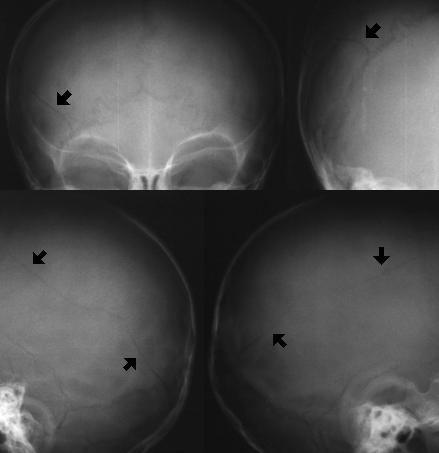
 This is a CT scan image. While this case has
focused on plain skull radiographs, CT scans are often
ordered in cases of significant head trauma.
Radiologists will usually read CT scans. Identification
of the sutures versus fractures on CT can be difficult
without the knowledge of the usual appearance and
location of sutures.
Case O Interpretation:
The top set of scans focuses on the brain which
appears to be normal. Extensive soft tissue swelling
exterior to the skull is evident on this set of scans.
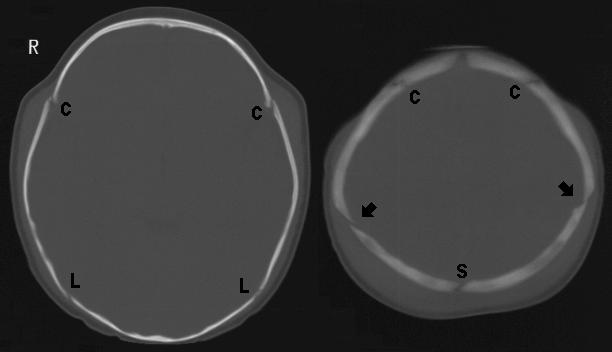
The lower set of scans is contrasted to view the
bones (bone windows). There are bilateral fractures of
the parietal region (arrows). The lambdoidal (L),
coronal (C), and sagittal (S) sutures are identified. Note
that the fracture is not seen in the lower cuts.
This is a CT scan image. While this case has
focused on plain skull radiographs, CT scans are often
ordered in cases of significant head trauma.
Radiologists will usually read CT scans. Identification
of the sutures versus fractures on CT can be difficult
without the knowledge of the usual appearance and
location of sutures.
Case O Interpretation:
The top set of scans focuses on the brain which
appears to be normal. Extensive soft tissue swelling
exterior to the skull is evident on this set of scans.
The lower set of scans is contrasted to view the
bones (bone windows). There are bilateral fractures of
the parietal region (arrows). The lambdoidal (L),
coronal (C), and sagittal (S) sutures are identified. Note
that the fracture is not seen in the lower cuts.
 View Case P.
View Case P.

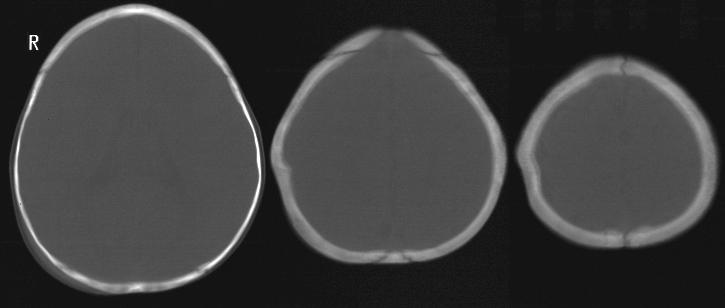 This is another CT scan case.
Case P Interpretation:
The top set of scans focuses on the brain which
appears to be normal. A skull depression is visible on
the right.
The lower set of scans is contrasted to view the
bones (bone windows). There is a depressed skull
fracture of the upper portion of the right parietal bone
(arrows). The lambdoidal (L) and coronal (C) sutures
are identified.
This is another CT scan case.
Case P Interpretation:
The top set of scans focuses on the brain which
appears to be normal. A skull depression is visible on
the right.
The lower set of scans is contrasted to view the
bones (bone windows). There is a depressed skull
fracture of the upper portion of the right parietal bone
(arrows). The lambdoidal (L) and coronal (C) sutures
are identified.
 References:
Bruce DA. Head Trauma. In: Fleisher GR, Ludwig
S. Textbook of Pediatric Emergency Medicine, third
edition. Baltimore, Williams & Wilkins, 1993, pp.
1105-1107.
The Head. In: Swischuk LE. Emergency Imaging
of the Acutely Ill or Injured Child, third edition.
Baltimore, Williams & Wilkins, 1994, pp 577-592.
References:
Bruce DA. Head Trauma. In: Fleisher GR, Ludwig
S. Textbook of Pediatric Emergency Medicine, third
edition. Baltimore, Williams & Wilkins, 1993, pp.
1105-1107.
The Head. In: Swischuk LE. Emergency Imaging
of the Acutely Ill or Injured Child, third edition.
Baltimore, Williams & Wilkins, 1994, pp 577-592.
Return to Radiology Cases In Ped Emerg Med Case Selection Page
Return to Univ. Hawaii Dept. Pediatrics Home Page