Abdominal Pain with a Negative Abdominal Examination
Radiology Cases in Pediatric Emergency Medicine
Volume 1, Case 3
Loren G. Yamamoto, MD, MPH
Kapiolani Medical Center For Women And Children
University of Hawaii John A. Burns School of Medicine
A 6 year old male presents to the ED with a chief
complaint of fever and stomach pain since last night. It
is now 11:00 a.m. The temperature was not measured
at home but he felt warm. He was given an unspecified
dose of acetaminophen at 4:00 a.m. There was no
history of nausea, vomiting, or diarrhea. His last bowel
movement was three days ago. He pointed to his
epigastrium as the location of most of his pain.
Exam: VS T38 (tympanic), P136, R24, BP 113/61.
He was noted to be small for age (19.3 kg), alert,
active, in no distress. He did not appear to be
uncomfortable at all. HEENT exam was unremarkable.
Neck supple without adenopathy. Heart regular without
murmurs. Lungs clear. Abdominal exam was positive
for mild tenderness in the epigastrium. Bowel sounds
were active. No tenderness in the right lower quadrant.
No rebound tenderness. No hepatosplenomegaly or
masses were appreciated. Testes were normal. A
rectal exam revealed normal sphincter tone, no
masses, and no right lower quadrant tenderness. The
stool tested negative for occult blood. An abdominal
series was ordered. An AP view of the chest was also
ordered as part of the abdominal series.
View abdominal series: Flat (Supine) view
 View abdominal series: Upright view
View abdominal series: Upright view
 View AP chest:
View AP chest:
 The radiographs were interpreted as showing
non-specific findings. Because the cause of the
abdominal pain was suspected to be constipation, the
patient was given an enema. Following this, he passed
a large amount of stool and felt much better. His
abdominal exam continued to be benign. He was
discharged from the ED. Overnight, the patient
continued to experience fever at home and some
abdominal pain though the degree of abdominal pain
was improved. A review of his radiographs the
following morning revealed an alternative diagnosis for
his symptoms.
Review his abdominal series again above.
If you are still unable to identify the radiographic
diagnosis, review the focused enlarged view of the
lesion.
The radiographs were interpreted as showing
non-specific findings. Because the cause of the
abdominal pain was suspected to be constipation, the
patient was given an enema. Following this, he passed
a large amount of stool and felt much better. His
abdominal exam continued to be benign. He was
discharged from the ED. Overnight, the patient
continued to experience fever at home and some
abdominal pain though the degree of abdominal pain
was improved. A review of his radiographs the
following morning revealed an alternative diagnosis for
his symptoms.
Review his abdominal series again above.
If you are still unable to identify the radiographic
diagnosis, review the focused enlarged view of the
lesion.
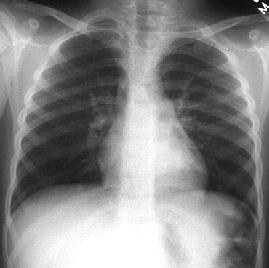
 This view provides a focused view of the lesion.
Note the triangular density superimposed on the heart.
The flat (supine) view shows this best (see below).
It is located at the very top of the flat (supine view).
This represents a pulmonary infiltrate in the medial
aspect of the left lower lobe. The top of it is cut off in
the flat (supine) view of the abdomen. It is almost
impossible to appreciate this density on the upright view
because most of it is cut off. The chest radiograph was
taken using a different degree of penetration to view the
lungs better. Because of this, it is even more difficult to
appreciate the infiltrate behind the heart. Upon close
inspection, you should be able to appreciate the
triangular density superimposed on the heart on the
chest radiograph view. A lateral view of the chest was
not taken in this case since the chest view was part of
an abdominal series that was ordered.
The patient was placed on antibiotics and his fever
promptly improved by the next day. His abdominal pain
and his other symptoms gradually improved.
Discussion and Teaching Points:
Pneumonia is a known cause of abdominal pain.
This diagnosis is often not considered because the
abdominal pain is the chief complaint. The pain can be
very severe at times. This can easily mislead a
clinician to limit the area of investigation to the
abdomen. This pitfall should be avoided. Causes of
abdominal pain that are not related to the abdomen
include pneumonia, pneumothorax,
pneumomediastinum, pericarditis, zoster, vertebral
conditions (eg., osteomyelitis, discitis), diabetic
ketoacidosis, etc. Adult conditions that are less likely
but still possible in children include myocardial ischemia
and aortic dissection.
Pulmonary conditions should be considered in
patients with respiratory symptoms, tachypnea, or a
borderline oxygen saturation. Documentation of these
findings should be routine in patients with abdominal
pain. The history should include the presence of and
the severity of respiratory symptoms. The vital signs
should include a respiratory rate and a pulse oximetry
reading. The examination should include notes
describing the presence or absence of any observed
tachypnea, the degree of coughing observed, the
characteristics of the cough (eg., moist, productive,
bronchospastic, dry, etc.), and the standard pulmonary
auscultation and percussion findings. If any of these
findings suggest the possibility of pneumonia, PA and
lateral chest radiographs should be ordered, or
alternatively, treatment prescribed for a clinical
diagnosis of a respiratory infection.
Although the likelihood of aortic dissection is low
(especially in children), this condition is associated with
a substantial likelihood of death which may be
preventable if the diagnosis is suspected early. While
aortic contrast studies by CT or aortography are not
routine, one suggestion has been to document the
presence and character of peripheral pulses in all
patients presenting with abdominal pain.
Although the appendix is often the focus of clinical
examination in patients with abdominal pain, there are
other serious causes of abdominal pain that should be
considered as well, such as intussusception, volvulus,
pancreatitis, ovarian torsion, testicular torsion, acute
cholecystitis, etc.
The radiographic findings in intussusception may
range from normal to various indirect signs of
intussusception (refer to Case 2 which describes the
radiographic findings in intussusception). A volvulus
is usually associated with a true bowel obstruction, but
the presentation clinically and radiographically can
occasionally be subtle.
Ovarian torsion may be a difficult diagnosis to make.
Even the use of color flow doppler ultrasound used to
assess blood flow to the ovaries is not able to totally
rule out this diagnosis since, early in its presentation,
some blood flow may still be preserved.
Testicular torsion is usually suspected on clinical
grounds, but occasionally the testes are not examined
in some patients because their pants and underwear (or
diapers) are not removed. Younger patients may fail to
point to their testes as the location of the pain. Some
may complain of non-specific abdominal pain because
of failure to appreciate the source of the pain, or
because of modesty.
In summary, the causes of abdominal pain are
extensive. In the acute care setting, it is most important
to rule out diagnoses that must be made early to result
in the best possible outcome for the patient. Some of
these diagnoses have been mentioned, but there are
others.
This view provides a focused view of the lesion.
Note the triangular density superimposed on the heart.
The flat (supine) view shows this best (see below).
It is located at the very top of the flat (supine view).
This represents a pulmonary infiltrate in the medial
aspect of the left lower lobe. The top of it is cut off in
the flat (supine) view of the abdomen. It is almost
impossible to appreciate this density on the upright view
because most of it is cut off. The chest radiograph was
taken using a different degree of penetration to view the
lungs better. Because of this, it is even more difficult to
appreciate the infiltrate behind the heart. Upon close
inspection, you should be able to appreciate the
triangular density superimposed on the heart on the
chest radiograph view. A lateral view of the chest was
not taken in this case since the chest view was part of
an abdominal series that was ordered.
The patient was placed on antibiotics and his fever
promptly improved by the next day. His abdominal pain
and his other symptoms gradually improved.
Discussion and Teaching Points:
Pneumonia is a known cause of abdominal pain.
This diagnosis is often not considered because the
abdominal pain is the chief complaint. The pain can be
very severe at times. This can easily mislead a
clinician to limit the area of investigation to the
abdomen. This pitfall should be avoided. Causes of
abdominal pain that are not related to the abdomen
include pneumonia, pneumothorax,
pneumomediastinum, pericarditis, zoster, vertebral
conditions (eg., osteomyelitis, discitis), diabetic
ketoacidosis, etc. Adult conditions that are less likely
but still possible in children include myocardial ischemia
and aortic dissection.
Pulmonary conditions should be considered in
patients with respiratory symptoms, tachypnea, or a
borderline oxygen saturation. Documentation of these
findings should be routine in patients with abdominal
pain. The history should include the presence of and
the severity of respiratory symptoms. The vital signs
should include a respiratory rate and a pulse oximetry
reading. The examination should include notes
describing the presence or absence of any observed
tachypnea, the degree of coughing observed, the
characteristics of the cough (eg., moist, productive,
bronchospastic, dry, etc.), and the standard pulmonary
auscultation and percussion findings. If any of these
findings suggest the possibility of pneumonia, PA and
lateral chest radiographs should be ordered, or
alternatively, treatment prescribed for a clinical
diagnosis of a respiratory infection.
Although the likelihood of aortic dissection is low
(especially in children), this condition is associated with
a substantial likelihood of death which may be
preventable if the diagnosis is suspected early. While
aortic contrast studies by CT or aortography are not
routine, one suggestion has been to document the
presence and character of peripheral pulses in all
patients presenting with abdominal pain.
Although the appendix is often the focus of clinical
examination in patients with abdominal pain, there are
other serious causes of abdominal pain that should be
considered as well, such as intussusception, volvulus,
pancreatitis, ovarian torsion, testicular torsion, acute
cholecystitis, etc.
The radiographic findings in intussusception may
range from normal to various indirect signs of
intussusception (refer to Case 2 which describes the
radiographic findings in intussusception). A volvulus
is usually associated with a true bowel obstruction, but
the presentation clinically and radiographically can
occasionally be subtle.
Ovarian torsion may be a difficult diagnosis to make.
Even the use of color flow doppler ultrasound used to
assess blood flow to the ovaries is not able to totally
rule out this diagnosis since, early in its presentation,
some blood flow may still be preserved.
Testicular torsion is usually suspected on clinical
grounds, but occasionally the testes are not examined
in some patients because their pants and underwear (or
diapers) are not removed. Younger patients may fail to
point to their testes as the location of the pain. Some
may complain of non-specific abdominal pain because
of failure to appreciate the source of the pain, or
because of modesty.
In summary, the causes of abdominal pain are
extensive. In the acute care setting, it is most important
to rule out diagnoses that must be made early to result
in the best possible outcome for the patient. Some of
these diagnoses have been mentioned, but there are
others.
Return to Radiology Cases In Ped Emerg Med Case Selection Page
Return to Univ. Hawaii Dept. Pediatrics Home Page